Andrew Lees
@ajlees
7,905
Followers
991
Following
1,347
Media
7,641
Statuses
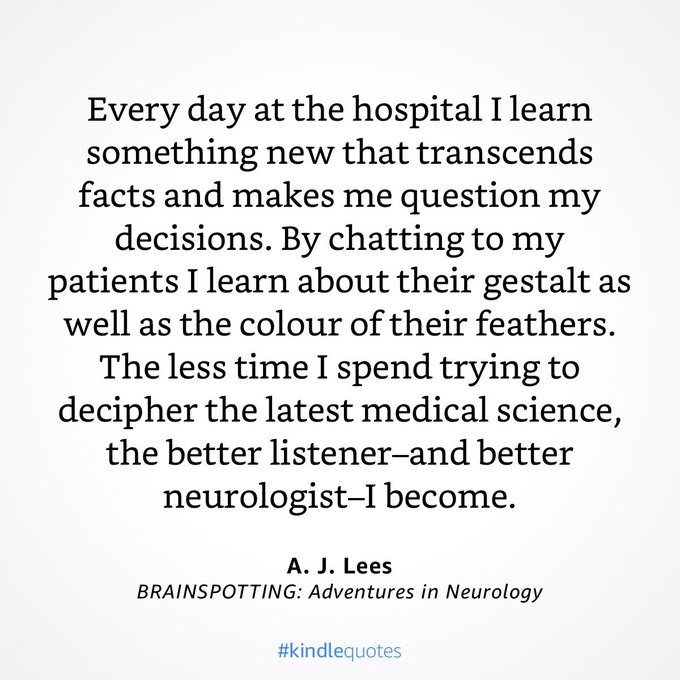
Professor of Neurology at UC London Author of Ray Kennedy biography, Liverpool:The Hurricane Port, Mentored by a Madman, Brazil that Never Was and Brainspotting
Don't wanna be here?
Send us removal request.