Andrew J
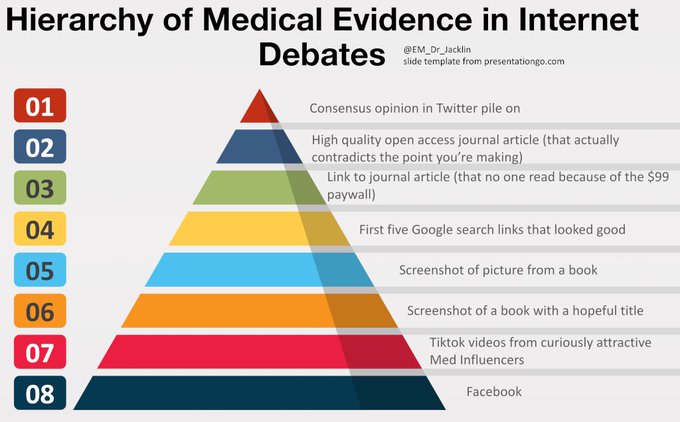
@EM_Dr_Jacklin
2,038
Followers
746
Following
837
Media
9,352
Statuses
Emergency Medicine Consultant, East Midlands. Trying to avoid drama, trying to generate some worthwhile discussions. May fail.
Derby
Joined March 2009
Don't wanna be here?
Send us removal request.