
PPP - Putting Patients First
@pppforpatients
7,823
Followers
2,155
Following
766
Media
7,523
Statuses
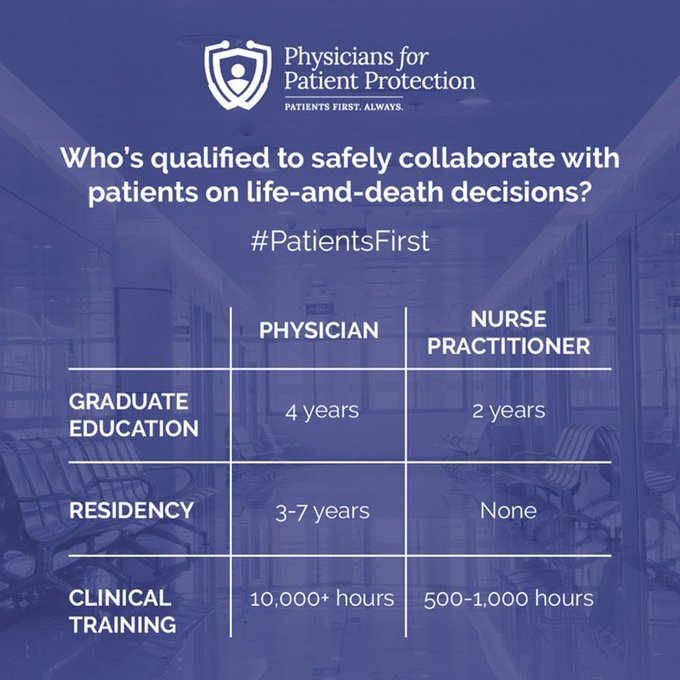
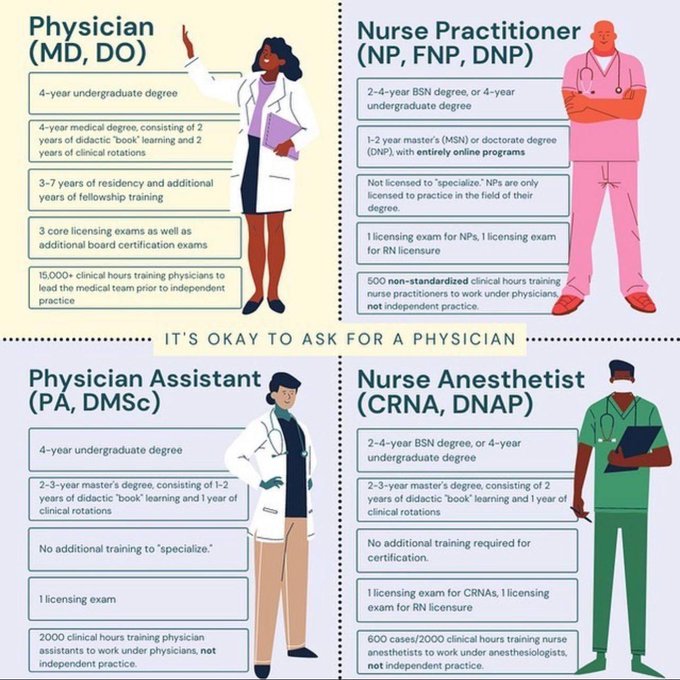
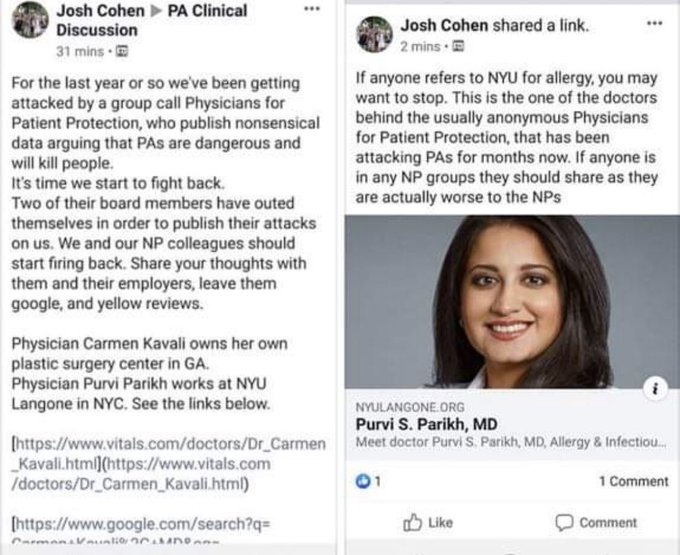
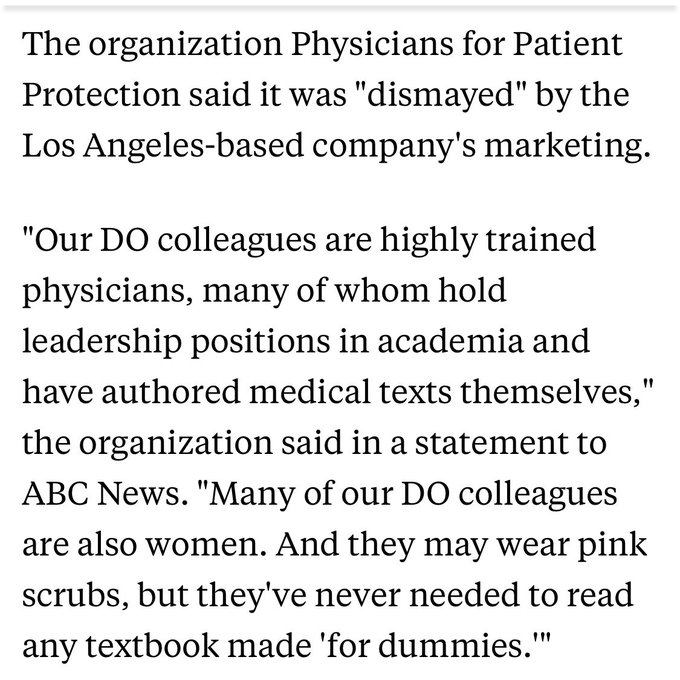
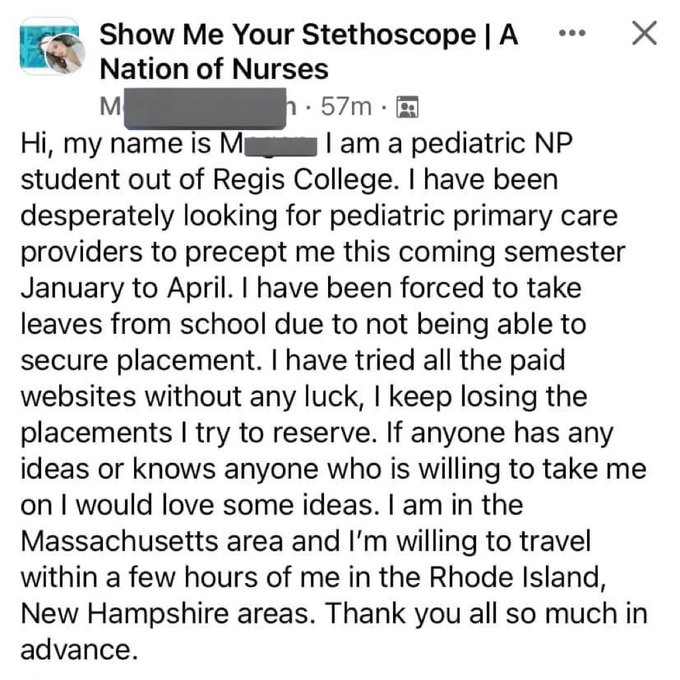
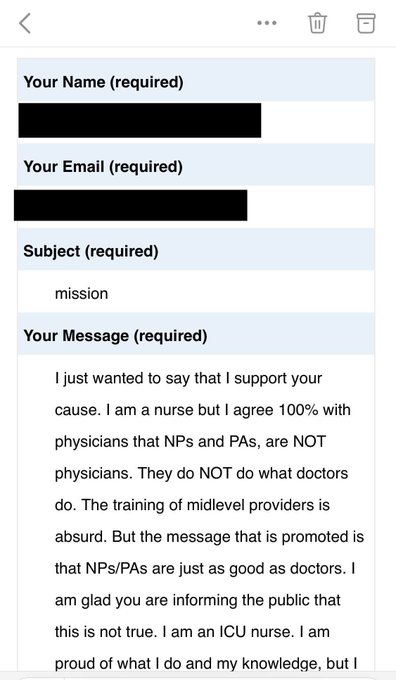
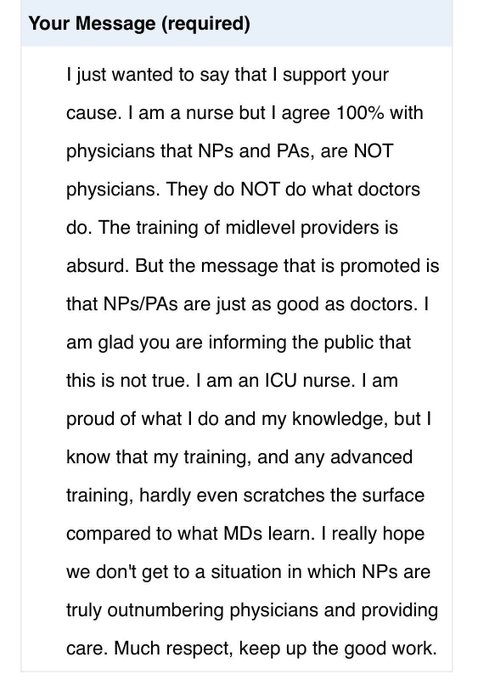
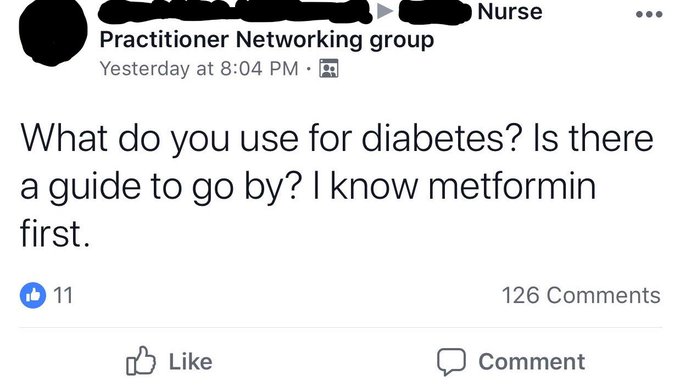
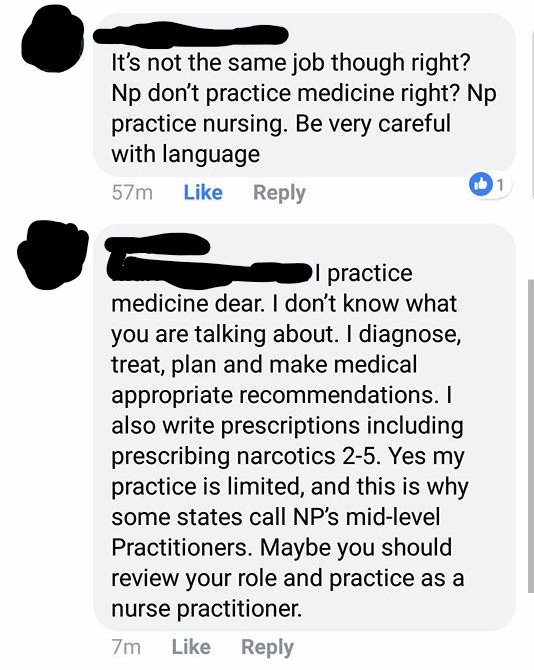
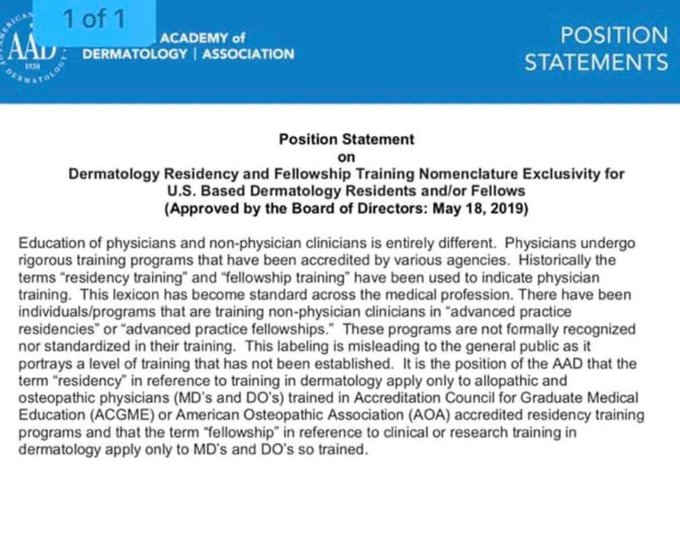
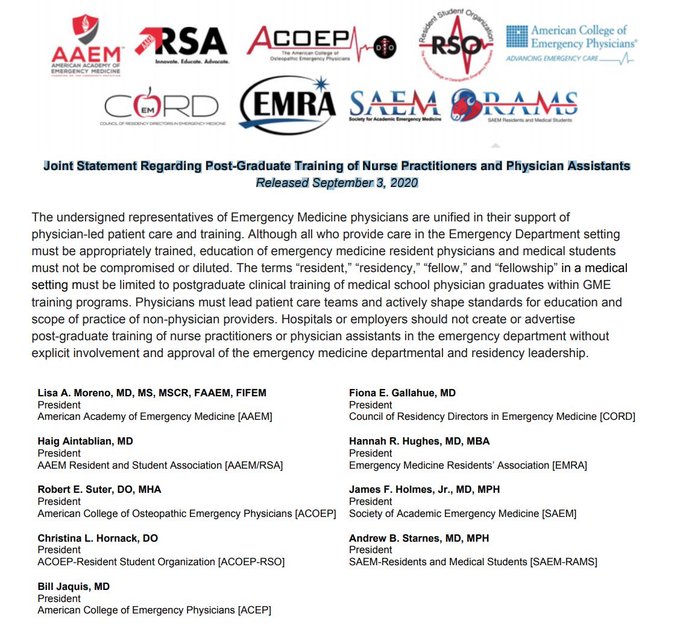
Physicians for Patient Protection: Ensuring physician-led care for all patients, and promoting truth and transparency regarding healthcare practitioners.
Don't wanna be here?
Send us removal request.