Evandro Martins F. MD
@evandrofilhobr
17,154
Followers
1,645
Following
3,478
Media
15,665
Statuses
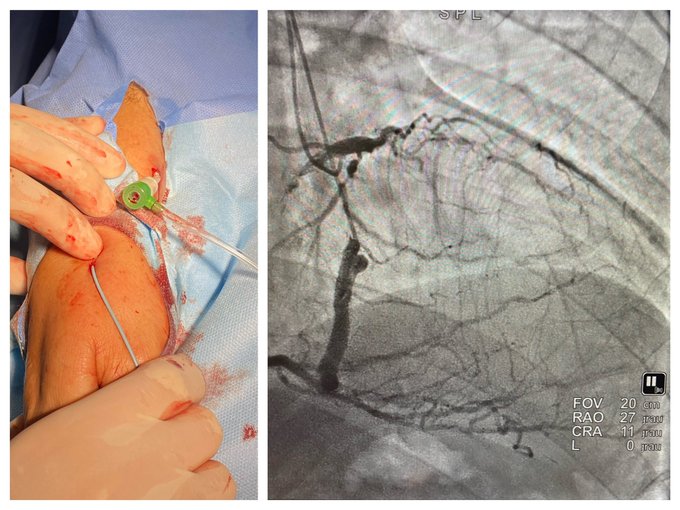
🇧🇷Interventional Cardiologist #RadialFirst #CTO #imagefirst Tweets=own opinion≠Medical advice. Freestyle proceduralist passioned to make people feel better!
Don't wanna be here?
Send us removal request.