JP 🍩🏀
@PoetryofAfter
4,346
Followers
2,621
Following
1,214
Media
17,385
Statuses
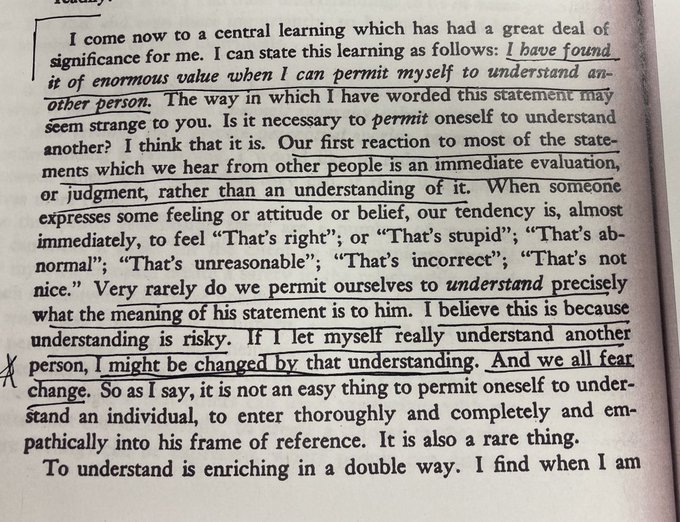
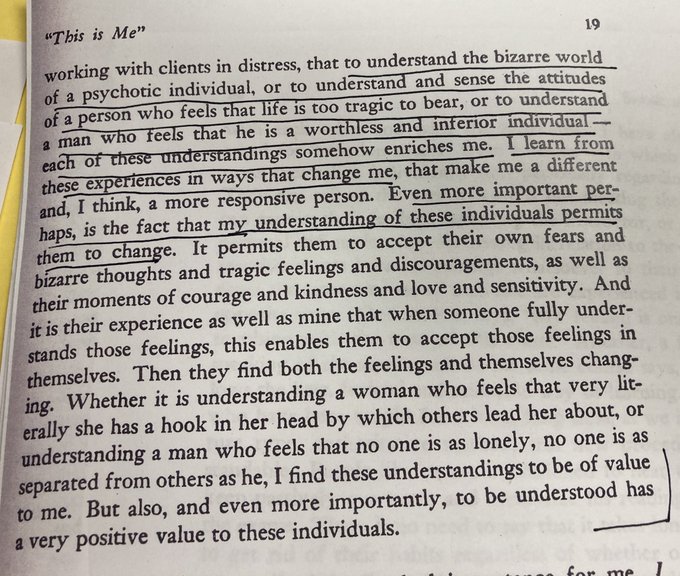
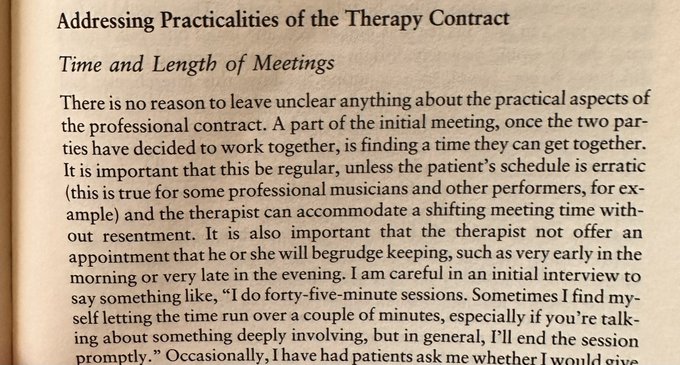
Psychotherapy. Psychoanalysis. Warriors. my tweets are impressions of the struggles, and evolutions of my learning, which is realizing how much I don’t know.
California, USA
Joined June 2011
Don't wanna be here?
Send us removal request.