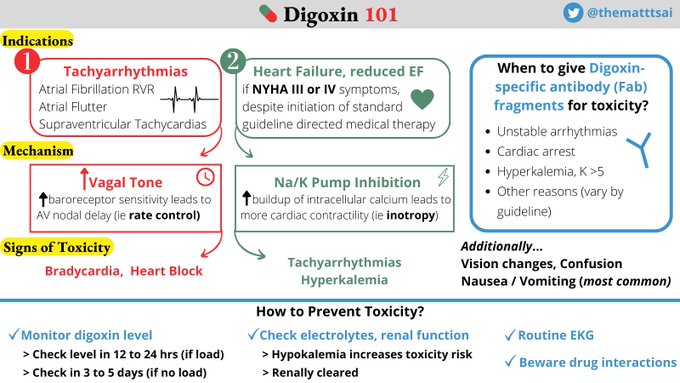
The good news is we have a targeted antidote: Digoxin specific antibody fragments!
Indications for this include unstable arrhythmias and hyperkalemia >5. /9
1
2
30
Replies
Took some time last week to focus on my own learning gaps regarding DIGOXIN 💊
What are its 2 main indications?
How does it work for those indications?
How do we monitor toxicity and how do we treat?
This is what I've learned, in a tweetorial🧵(graphic at the end!) /1
11
166
638
First, which is NOT an indication for Digoxin? /2
Rate control afib/flutter
226
HFrEF NYHA III or IV
693
Arrhythmia rhythm control
982
Rate control of SVT
1352
1
1
11
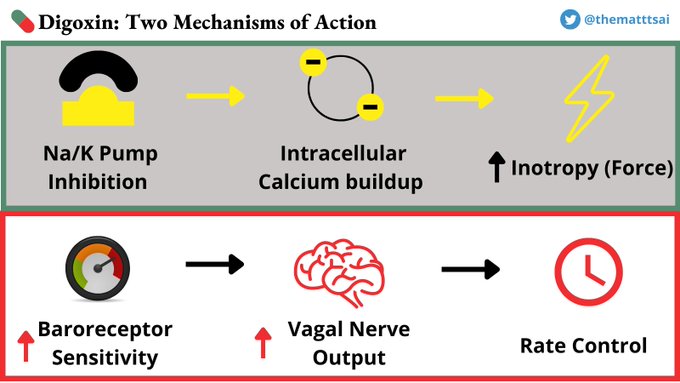
Indications for Digoxin are twofold.
The first is rate control for certain tachy-arrhythmias (afib, aflutter, SVT).
🧐But how does this happen? Does it increase... /3
Vagal Tone
305
Baroreceptor sensitivity
96
AV node refractory period
820
All of the above
1358
1
2
10
Digoxin indirectly⬆️baroreceptor sensitivity which ⬆️vagal tone, + prolongs AV node refractory period! This works best when pts are sedentary.
Making Dig a rate control option in atrial or supraventricular tachycardias, esp in decompensated HF when BB or CCB contraindicated /4
1
7
56
The second (less common) indication for digoxin:
HFrEF with NYHA III or IV symptomatology (ie severe symptoms with exertion or symptoms at rest).
🚨Caveat: this is a second-line agent, to be considered AFTER all standard GDMT /5
2
2
28
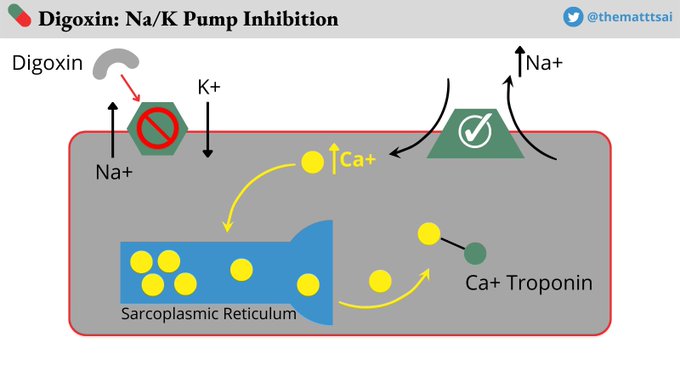
This relates to digoxin's more well-known mechanism, inhibition of the Na/K ATPase Pump! This process drives up intracellular calcium stores, which⬆️ inotropy.
In other words, digoxin is a potential inotropic agent in HFrEF with NYHA III/IV symptoms despite standard GDMT /6
1
5
31
So we have talked about mechanisms and indications, but what about safety profile? Which is NOT a sign of digoxin toxicity? /7
Hypokalemia
979
Heart Block
111
Tachyarrhythmias
631
Vision changes
166
1
1
7
Digoxin Toxicity presents as:
Hyperkalemia - because it ❌ the Na/K pump
Bradycardia or heart block - because ⬆️vagal tone
Tachyarrhythmias because of its inotropic effect ⚡️
GI Upset (most common), Vision changes
If we are concerned for toxicity, how would we treat? /8
2
5
34
Obviously, prevention is🔑 How?
✅Check digoxin level (does not correlate to toxicity well, but can determine compliance)
🧪Check electrolytes (hypoK ⬆️toxicity risk)
🚨Beware drug interaction
🫘 Monitor kidney fx (hence digoxin less commonly used outpt)
❤️EKG, telemetry /10
2
2
25
In summary:
We started with 3 questions.
❓Digoxin indications
❓Mechanism(s)
❓Sx and Rx of Toxicity
Take a moment to recall what we covered. Answers (in a graphic!) next.
Thank you to
@AdamRodmanMD
and
@ShreyaTrivediMD
and
@jasonmatosmd
for their feedback on this🧵! /end
1
2
19