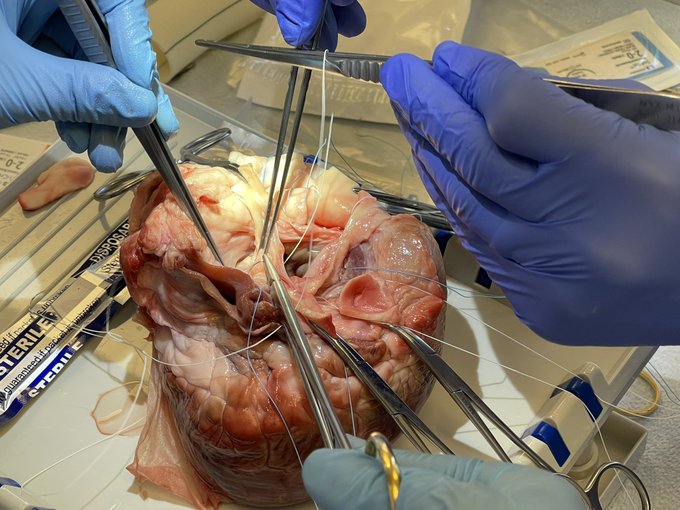

Phillip Rowse, MD, FACS
@RowseMD
3,738
Followers
314
Following
187
Media
354
Statuses
Cardiac Surgeon - Mayo Clinic, Robotic Enthusiast, Rock Climber, Educator, tweets are my own.
Rochester, MN
Joined July 2013
Don't wanna be here?
Send us removal request.